Temporary Anchorage Device (TAD) use in the treatment of anterior open bite
Article by Padraig Dennehy, DMD | Featured on Dentistry IQ
This article first appeared in the newsletter, DE’s Breakthrough Clinical with Stacey Simmons, DDS.
While orthognathic surgery is sometimes the only option for treatment of certain skeletal malocclusions, having another tool in the orthodontist’s arsenal is a welcome option for patients and clinicians alike. Anterior open bite, defined as a state in which the maxillary and mandibular molars occlude first in mandibular closure, leaving the anterior teeth out of contact (1), has previously been treated by a variety of means. These treatments include but are not limited to extractions, high-pull headgear, bite blocks, elastics, and functional appliances (2). In more severe cases, the patient may require orthognathic surgery to correct the skeletal malocclusion. In cases of anterior open bite due to overeruption of the maxillary posterior teeth (posterior maxillary vertical excess), the oral surgeon will reposition the posterior maxilla superiorly, allowing autorotation of the mandible upward and forward to close the open bite (2). Orthognathic surgery is a predictable treatment modality for anterior open bite cases, but is sometimes cost prohibitive and has associated risks and recovery time.
ADDITIONAL READING | Treatment considerations for the congenitally missing maxillary lateral incisor
Recently, the minimally invasive placement of TADs (temporary anchorage devices) has allowed orthodontists to treat some of these patients without orthognathic surgery through intrusion of the posterior maxillary molars. While TADs are not a substitute for surgery in all cases, they do provide a treatment alternative for specific mild-to-moderate open bite cases without other skeletal malformations.
TADs are titanium-alloy mini-screws that range from 6–12 mm in length and 1.2–2 mm in diameter (3). The orthodontist or surgeon can insert the TAD directly into the bone through the gingiva with a handheld driver and, most often, with the use of only topical anesthetic (3). The TAD can be loaded immediately as it gains its anchorage through mechanical gripping of bone rather than through osseointegration (3).
ADDITIONAL READING | Orthodontic options for the ectopic eruption of a maxillary first molar
In the case of anterior open bites, TADs are placed bilaterally on the buccal aspect of the maxilla between the second premolar and first molar. The greatest amount of interradicular bone in the posterior maxilla is found in this region, about 5–8 mm from the alveolar crest (3). In the case of less-than-ideal interradicular bone, the TAD could be placed palatally or roots can be diverged before TAD placement (3). The maxillary molars and premolars are banded and bracketed respectively and ligated with bilateral, segmented stainless steel wires. Once levelling and aligning of these teeth are complete, the TAD is placed and a nickel titanium coil and elastic chain are used to connect the TAD to the mesial of the first premolar and hook of the second molar band. This creates a light and continuous force to produce intrusion en masse of the first premolar to the second molar bilaterally.
In conjunction with TAD placement, a TPA (transpalatal appliance) is placed to prevent the intruding molars and premolars from tipping buccally (3). An acrylic button is placed on the center of the TPA and the patient is instructed to press occasionally on the button with the tongue. Tongue pressure on the TPA also aids in tooth intrusion (3).
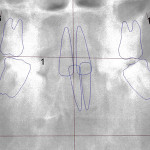
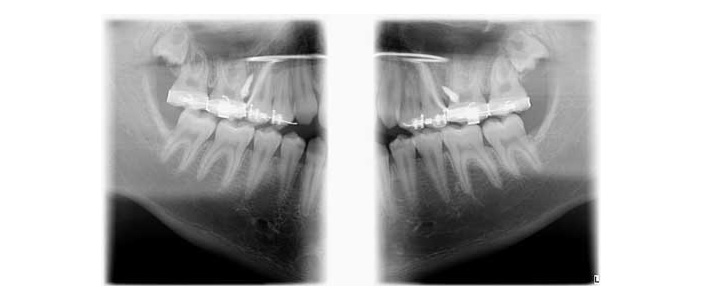
Case report
A healthy 15-year-old male presents to the clinic with an anterior open bite. His case is outlined in the figures below.





The patient in the above case report is still in active treatment. Now that successful maxillary posterior intrusion has been accomplished, the remaining full, fixed orthodontic appliances can be placed. The TPA can be removed and the molar intrusion will be held for the remainder of treatment with a ligature tie placed from the first molar to the TADs. The TADs will be kept in place for the remainder of treatment to maintain the stability of the intrusion as bone remodeling occurs.
In terms of stability of anterior open bite treatment using TADs to intrude the posterior maxillary teeth, a study by Baek et al. showed that the relapse of the incisal overbite was 17% in the first year post deband (4). Three year follow-up was done on these same patients and no further significant relapse was noted (4). Thus, relapse appears to be most common during that first year, and as such an appropriate retention protocol with strong patient compliance is important in terms of outcome of this treatment.
More studies are needed to determine whether treatment of anterior open bites with TADs will stand the test of time, but what is known for sure is that if given the option, many patients will benefit from this nonsurgical approach as a viable treatment option for their malocclusion.
This article first appeared in the newsletter, DE’s Breakthrough Clinical with Stacey Simmons, DDS.
 Padraig Dennehy, DMD, is a fourth-generation Montanan, having been born and raised in Butte, Montana. He attended Montana Tech of the University of Montana, graduating summa cum laude with a major in biology and a minor in mathematics. Dr. Dennehy obtained his dental degree from Harvard School of Dental Medicine in June 2007. Following Harvard, he completed a two-year residency program in the specialty of orthodontics at the University of Minnesota. Prior to returning to Montana, he practiced orthodontics in Minnesota for two years. He is a member of the cleft lip and palate team, working in conjunction with other professionals to treat craniofacial patients who require specialized care. When he is not treating patients, Dr. Dennehy enjoys playing tennis, racquetball, mountain biking, hiking, trivia, and playing with his Siberian Husky, Dublin.
Padraig Dennehy, DMD, is a fourth-generation Montanan, having been born and raised in Butte, Montana. He attended Montana Tech of the University of Montana, graduating summa cum laude with a major in biology and a minor in mathematics. Dr. Dennehy obtained his dental degree from Harvard School of Dental Medicine in June 2007. Following Harvard, he completed a two-year residency program in the specialty of orthodontics at the University of Minnesota. Prior to returning to Montana, he practiced orthodontics in Minnesota for two years. He is a member of the cleft lip and palate team, working in conjunction with other professionals to treat craniofacial patients who require specialized care. When he is not treating patients, Dr. Dennehy enjoys playing tennis, racquetball, mountain biking, hiking, trivia, and playing with his Siberian Husky, Dublin.
References
1. Paik CH. Molar intrusion using TADs: The key element to correcting anterior open bite and/or vertical excess problems. AAO Annual Session, Philadelphia. May 5, 2013. Lecture.
2. Scheffler NR, Proffit WR, Phillips C. Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am J Orthod Dentofacial Orthop. Nov. 2014;146(5):594-602.
3. Kravitz ND, Kusnoto B, Tsay TP, Hohlt WF. The use of temporary anchorage devices for molar intrusion. JADA. Jan 2007;138:57-64.
4. Baek MK, Choi YJ, Yu HS, Lee KJ, Kwak J, Park YC. Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. Oct. 2010;138(4):396.e1-9; discussion 396-8. doi: 10.1016/j.ajodo.2010.04.023.
Looking for an orthodontist in Beaverton, Oregon? Biermann Orthodontics is a cutting-edge orthodontic practice that serves Beaverton and Molalla, OR, and focuses on providing world-class customer service and efficient treatment. We strive to create stunning smiles in the shortest amount of time without ever sacrificing quality.
Visit our Locations page to find a clinic near you, or schedule an initial consultation.
Biermann Orthodontics
503-690-0722
17885 NW Evergreen Parkway, Suite 200
Beaverton, OR 97006